
Gulf Coast Pain Consultants paid $1.19 million to OCR in December 2024. The underlying issue wasn't a sophisticated attack. A contractor had unauthorized access to the practice's EMR for five months. The practice didn't conduct a risk analysis until three years after the breach. It didn't review access logs. It didn't terminate the contractor's access when it should have.
The root cause is older and more common than any of these individual failures: the patient data that was accessed was unencrypted, living in a system whose access controls hadn't been reviewed, outside the tight security model the EHR vendor built for records in active clinical use.
This is the shadow PHI problem. And every healthcare organization with an EHR has it.
Is Your Security Program Stopping at the EHR Boundary?
OCR is now auditing "Risk Management", not just analysis. If you can't see your shadow PHI, you can't manage the risk.
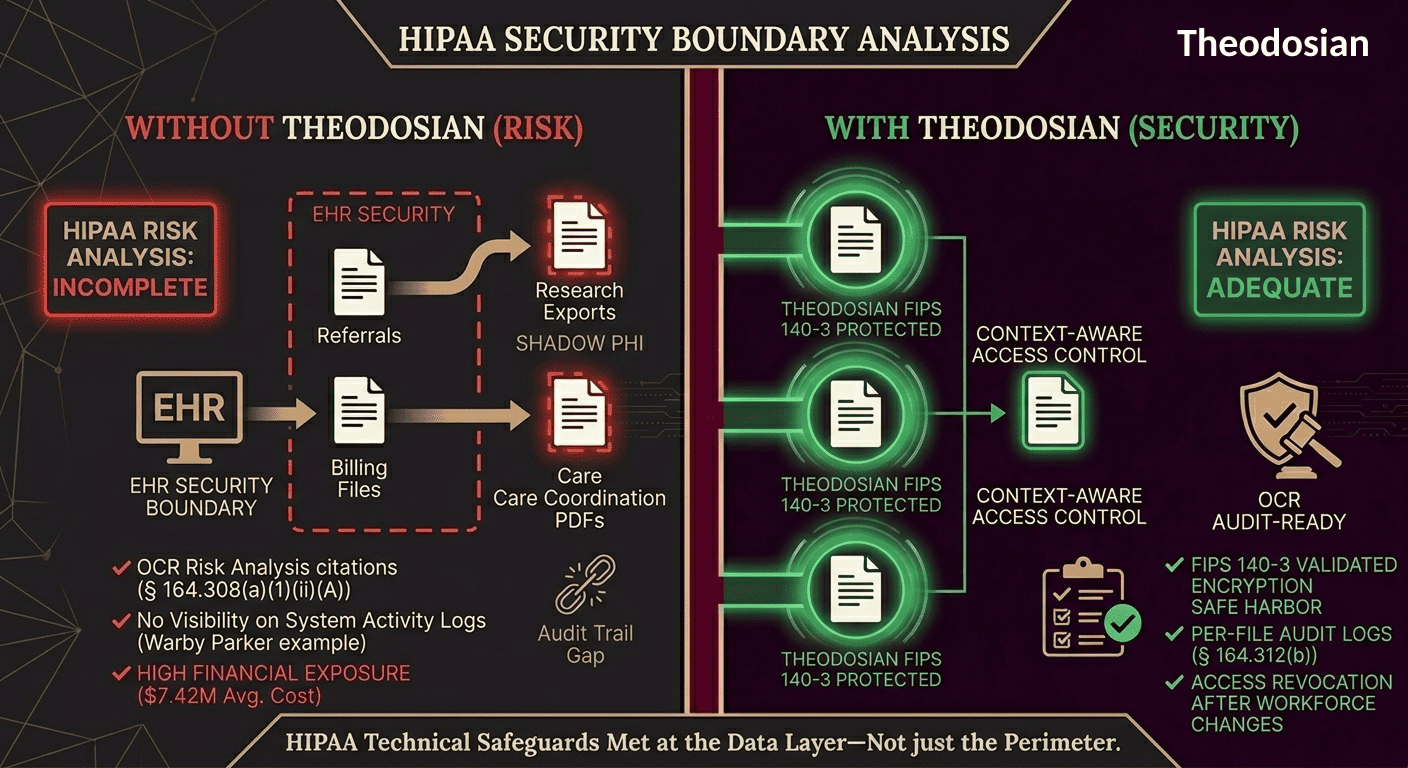
What Your EHR Protects
Electronic health record systems are purpose-built for clinical workflows. They authenticate users, enforce role-based access, maintain audit trails, and — for records inside the system — provide a well-governed security environment.
The protections are real, but they have a hard boundary: the EHR protects records while they live inside it.
From the moment a record moves — exported to a PDF, attached to a referral, pulled into a billing file, shared with a specialist, handed to an attorney for a legal hold — the EHR's security model ends. What happens to that file afterward depends entirely on the security posture of wherever it goes next.
In most healthcare organizations, that answer is: not much.
What Shadow PHI Is
Shadow PHI is protected health information that exists outside officially monitored systems — scattered across email inboxes, file shares, personal cloud accounts, legacy servers, vendor platforms, and backup archives. It's not hidden maliciously. It accumulates through normal clinical and administrative workflow.
A few common examples:
Referral documents: A primary care physician sends a specialist a patient summary as a PDF attachment over unencrypted email. The file is now on the specialist's email server, potentially forwarded, possibly backed up, and entirely outside any governance framework.
Billing and insurance files: Claims, explanation of benefits documents, and pre-authorization records flow to insurers, third-party billing vendors, and revenue cycle management companies. Each handoff is a new, unmonitored location for the same patient data.
Research exports: Lab results, imaging data, and de-identified (or inadequately de-identified) datasets get pulled into spreadsheets for research partnerships. The EHR audit log recorded the export. It has no visibility into what happened to the spreadsheet.
Legal holds: When litigation places a healthcare organization under a document preservation obligation, PHI gets collected into file repositories that may sit outside normal security monitoring for years.
Care coordination: Discharge summaries, transition of care documents, and specialist notes move between facilities, providers, and sometimes patients themselves — often by email, often unencrypted.
Vendor integrations: Analytics platforms, imaging systems, and EHR integrations create copies of PHI on servers that aren't part of the main EMR security model. As Healthcare Dive reported in 2025, "much of the unencrypted data in 2025 breaches existed outside the electronic health record: on analytics servers, imaging platforms, email systems, and vendor integrations where encryption enforcement was inconsistent or absent."
Every one of these represents a file carrying protected health information, traveling through channels the EHR was never designed to protect.
Why This Creates Specific HIPAA Exposure
HIPAA's Technical Safeguards standard at 45 CFR § 164.312 requires covered entities to implement technical security measures for electronic PHI. The requirements apply to ePHI wherever it exists — not just within the EHR.
The specific gap shadow PHI creates:
Access Control (§ 164.312(a)) requires unique user identification and emergency access procedures, with addressable specifications including automatic logoff and encryption/decryption mechanisms. These controls are enforceable inside the EHR. Outside it, on a file sitting in a billing vendor's archive, they don't exist.
Audit Controls (§ 164.312(b)) require hardware, software, or procedural mechanisms to record and examine activity in systems containing ePHI. A file emailed to a specialist is in a system that likely has no HIPAA audit controls at all.
Transmission Security (§ 164.312(e)) requires technical measures guarding against unauthorized access to ePHI transmitted over electronic networks — with encryption as an addressable specification. An email without encryption fails this requirement when it carries PHI.
The critical enforcement reality: OCR doesn't only audit your EHR. It audits your information security program — which is supposed to cover all ePHI, everywhere. A risk analysis that stops at the EHR boundary is an incomplete risk analysis, and incomplete risk analyses are OCR's top enforcement target.
In 2026, OCR has expanded its enforcement initiative from risk analysis to risk management — meaning the agency is now scrutinizing whether organizations not only identify risks but actively remediate them. Shadow PHI that was never inventoried can't be managed.
The Numbers That Define the Risk
276.7 million healthcare records were breached in 2024 — the worst year ever recorded, representing a 64.1% increase from 2023. (Source: HIPAA Journal, 2026)
35.5% of 2024 healthcare breaches originated from third-party vendors — the very channel through which shadow PHI flows. (Source: HIPAA Journal)
The average healthcare data breach costs $7.42 million — the costliest of any industry for 14 consecutive years. (Source: IBM Cost of a Data Breach)
170 email breaches occurred in 2025, affecting 2.5 million individuals. Phishing is the number one access vector — and phishing targets email accounts where unencrypted PHI is routinely stored. (Source: HIPAA Journal)
43% of breaches are attributed to human error — including lost or stolen devices containing unencrypted downloaded records. (Source: HIPAA Journal)
The Encryption Safe Harbor, and Why Shadow PHI Can't Use It
HIPAA includes a meaningful protection for organizations that encrypt properly: the breach notification safe harbor.
Under 45 CFR § 164.402, encrypted ePHI is not considered "unsecured PHI," which means if encrypted data is lost, stolen, or accessed improperly, no breach notification is required. No OCR report. No patient notification. No fine. The incident is classified as a security event, not a reportable breach.
The condition: the encryption must meet HHS guidance using FIPS-validated cryptography, and the decryption key must not have been compromised alongside the data.
The problem with shadow PHI is that it typically isn't encrypted when it travels. A referral PDF sent by email isn't encrypted. A billing file shared with a third-party vendor via an unsecured file transfer isn't encrypted. A spreadsheet of research data on an analytics server isn't encrypted.
The safe harbor only applies to data that was actually encrypted. Shadow PHI, by its nature, usually isn't.
What Real PHI Protection at the File Level Looks Like
The gap isn't in the EHR. It's in everything that moves.
Per-file FIPS 140-3 validated encryption means every document carrying PHI has its own cryptographic key embedded within it — persistent protection that doesn't depend on the security posture of the email server, cloud storage, or vendor system it lands in.
Context-aware access controls extend the governance model beyond your perimeter. An authorized recipient can open the file. An unauthorized one — including an attacker with valid credentials from a phished account — cannot. Access is denied at the file itself, not at the network boundary.
If a device containing downloaded patient records is lost or stolen, access to those files can be revoked immediately and retroactively. The file becomes inaccessible on that device, regardless of where the device is located.
For OCR audit purposes, every access attempt — successful or denied — generates a per-file audit log entry. This is the kind of evidence that satisfies the § 164.312(b) audit control requirement: a record of activity on ePHI, at the file level, wherever the file lives.
This approach addresses HIPAA's Technical Safeguard requirements at the data layer — specifically the access control, audit control, integrity, and transmission security provisions of § 164.312. It's the layer that makes shadow PHI governable rather than invisible.
The Healthcare Security Checklist
The questions below map to OCR's audit protocol and the most common gaps that generate enforcement action. Use them to assess where your organization stands on shadow PHI and file-level security.
- Has your encryption implementation been assessed against FIPS-validated standards — the specific requirement for the HIPAA encryption safe harbor?
- When a workforce member or contractor's access is terminated, are all downloaded PHI files on their devices also revoked?
- Do you have audit logs covering file-level access to PHI outside the EHR?
- Can you revoke access to a PHI-containing document after it has been downloaded or forwarded?
- Are files containing PHI encrypted when transmitted by email, file transfer, or shared drive?
- Do your business associate agreements require service providers to implement encryption and access controls on PHI they receive?
- Do you have a current inventory of every third-party service provider that receives PHI from your organization?
- Does your risk analysis cover ePHI that exists outside the EHR — including email attachments, billing files, referral documents, and data at vendor locations?
If any answer is "no" or "we're not sure," those gaps represent both regulatory exposure and breach notification risk that the EHR's security model doesn't address.
Make Data Exposure a Non-Event
If your data is encrypted at the file level, a lost device or phished account isn't a reportable breach; it’s just a non-event. Secure the data, not just the perimeter.
FAQs: HIPAA File Security
Does HIPAA require encryption for all PHI files?
HIPAA classifies encryption as an "addressable" implementation specification under § 164.312, which means organizations must conduct a risk-based assessment and either implement encryption or document an equivalent alternative. However, encryption is the only mechanism that qualifies for the HIPAA breach notification safe harbor — if unencrypted PHI is lost or improperly accessed, notification to OCR, affected individuals, and potentially the media is required. Given the safe harbor's value and OCR's enforcement posture, treating encryption as a practical requirement is the defensible approach.
What is the HIPAA encryption safe harbor?
Under 45 CFR § 164.402, ePHI that has been rendered "unusable, unreadable, or indecipherable" through encryption meeting HHS guidance is not considered "unsecured PHI." This means a breach involving properly encrypted data does not trigger breach notification requirements — the incident is a security event, not a reportable breach. The safe harbor applies only when the decryption key was not also compromised. Files that are unencrypted — including most shadow PHI — do not qualify.
What do OCR auditors look for in file-level security?
OCR audit protocol under the Technical Safeguards standard requires documentation of encryption implementation, key management procedures (including rotation and revocation logs with a minimum 6-year retention), unique user identification policies with access logs, audit log evidence of activity monitoring for all ePHI, and evidence of access termination procedures. Auditors are specifically looking for whether written policies align with actual operations — not just whether policies exist on paper.
How does per-file encryption differ from encrypting the EHR?
EHR encryption protects records inside the system. Per-file encryption embeds a unique cryptographic key and access policy in each document itself — protection that travels with the file regardless of where it goes. A PHI file encrypted at the file level remains protected when downloaded to a personal device, forwarded outside the organization, shared with a vendor, or stored in any environment. The EHR's encryption ends when the file leaves; per-file encryption doesn't.
What are the most common HIPAA violations leading to OCR fines?
OCR's most frequently cited violation is failure to conduct an adequate risk analysis — appearing in the majority of recent enforcement actions. Related failures include not reviewing system activity logs (Gulf Coast Pain Consultants, $1.19 million), inadequate access controls after workforce changes, and failure to implement sufficient security measures following identified risks (Warby Parker, $1.5 million). In 2026, OCR has expanded enforcement to also target inadequate risk management — meaning organizations that identify risks but fail to remediate them.